Gender-Responsive Programming: Maternal and Child Health Policies & Programs for Female Offenders
This post serves as a review of Pendleton et al.’s (2020) research article, Corrections officers’ knowledge and perspectives of maternal and child health policies and programs for pregnant women in prison, as well as additional research and empirical literature on gender-responsive programming for female offenders within the carceral setting. In the past three decades, the number of women placed in prison and jails has increased more than 750%, which is a rate twice as high as men (Equal Justice Initiative, 2020). Dr. Rousseau argues that to “foster effective policy and programming,” it is imperative to recognize the diverse nature of prison populations. Further, asserting that the national rate of women’s incarceration has been rising drastically since the mid-1990s and early 2000s because of a shift to mass incarceration and a focus on punishment over rehabilitation (Rousseau, 2021). Despite the alarmingly high rate of women entering the carceral settings, many state and federal institutions severely lack gender-responsive programming to serve female offenders. As the female prison population has grown, Pendleton et al. (2020) note the growing need for gender-responsive policies and programs in carceral settings, including the development and implementation of programs that meet the unique needs of pregnant women in prison.
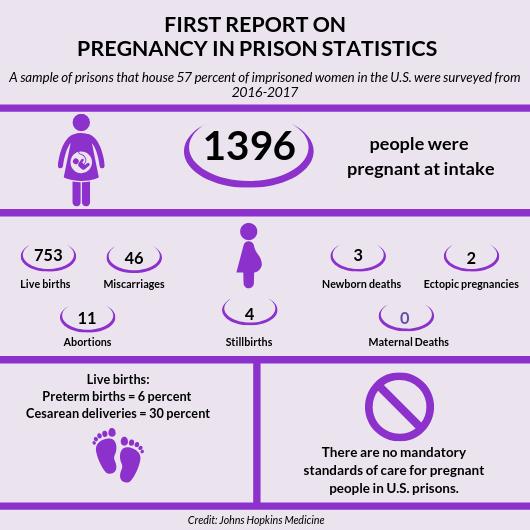
Perhaps most concerning is the limitation of services offered to pregnant inmates. Pendleton et al. (2020) assert that the United States has the largest population of incarcerated women globally, with 112,000 women housed in federal or state prisons and an additional 110,000 in jails (Pendleton et al., 2020). While national data regarding pregnancy is not routinely collected, recent studies argue that 3.8% of newly admitted women are pregnant, with nearly 1,400 women giving birth every year while incarcerated (Pendleton et al., 2020).
One of the more controversial practices against pregnant inmates is the use of shackles and restraints during labor and the birthing process. Of the more than 225,000 women incarcerated today, only 15% of them are housed in federal prison, where they are protected under the new federal prohibition on using restraints during pregnancy, labor, and postpartum recovery (Equal Justice Initiative, 2020). Ultimately, according to medical experts, the use of shackles poses a significant safety risk, including “the potential for injury or placental abruption caused by falls, delayed progress of labor caused by impaired mobility, and delayed receipt of emergency care when corrections officers must remove shackles to allow for assessment or intervention” (Equal Justice Initiative, 2020, 3). Furthermore, a 2017 report published by the American Psychological Association (APA) argues that the use of restraints during the transport of women to prenatal care and labor can obstruct necessary medical care. The risk of restraining female offenders is exacerbated during labor when the use of shackles can lead to an unnecessary amount of physical pain and increase the chance for complications due to the mother’s inability to move freely (Equal Justice Initiative, 2020).

Further, physicians have noted the increased difficulty, and, on occasion, their inability to “administer epidurals due to restraints, and in one documented case, a woman restrained during labor experienced a hip dislocation that caused permanent deformities and pain, stomach muscle tears, and an umbilical hernia” (Equal Justice Initiative, 2020, 4). In addition to the traumatic and painful physical effects, incarcerated women experience severe mental distress, with restrained women reporting depression and anguish, as well as the exacerbation of pregnancy-related mental health problems, including postpartum depression and post-traumatic stress disorder (Equal Justice Initiative, 2020). This is especially concerning according to the psychiatrist, Dr. Terry Kupers, who argues that incarcerated women have a greater propensity to have suffered from childhood traumas; and the experience of being shackled “can increase post-traumatic symptoms caused by prior experiences of trauma. This re-traumatizing experience, he said, ‘makes conditions like post-traumatic stress disorder much worse’” (Equal Justice Initiative, 2020, 7). This is supported by Pendleton et al. (2020), who asserts that “medical contraindications to the use of restraints include interfering with balance and increasing the risk of falls, causing delays during medical emergencies, limiting mobility which can make labor more difficult, and impeding mother and infant bonding” (Pendleton et al., 2020, 2).
Regarding the comparison to male inmates, Dr. Rousseau argues that women in prison have a higher likelihood of having a history of physical or sexual abuse. Further, they are usually the primary caretakers of young children or may even be pregnant when entering the criminal justice system or suffering from postpartum depression (Rousseau, 2021). Similarly, women entering the criminal justice system are at a heightened risk of facing serious mental illness in comparison to their male counterparts: “A larger percentage of women are diagnosed with major depression and anxiety disorders, especially PTSD. A majority of women in the system (up to 70%, possibly even more) report a history of abuse as a child or adult” (Rousseau, 2021, 4.5). Similarly, Kupers’ (1999) book “Prison Madness: The Mental Health Crisis Behind Bars and What We Must Do About It” argues that since a “significant proportion of women prisoners were sexually abused as children, and quite a few of this group have substance abuse problems, it is not surprising to find that many are depressed” (Kupers, 1999, 23). Ultimately, Kupers (1999) argues that the themes of “childhood abuse, domestic violence, drugs, and depression are omnipresent in the stories of women prisoners who suffer from serious psychiatric disorders” (Kupers, 1999, 24).

Despite the mounting and robust evidence of the danger to the mother and child, 23 states do not have laws prohibiting the use of shackles for incarcerated pregnant women, despite most women serving time for nonviolent offenses. A 2019 study suggests that pregnant incarcerated women are shackled far more often, finding that “83% of perinatal nurses who cared for incarcerated women during pregnancy, or the postpartum period reported that shackles were used on their patients sometimes to all of the time, and 12.3% reported that their patients were always shackled. In a third of cases, the only reason cited for shackling was adherence to a rule or protocol” (Equal Justice Initiative, 2020, 9).
Ultimately, while the same study found that corrections officers (COs) often assert that unrestrained incarcerated women pose flight or public safety risks, the APA argues that there is no record of escape for any unrestrained incarcerated women (Equal Justice Initiative, 2020). The role of the CO is significant to determine gender-responsive strategies for pregnant women. As the largest occupational group within prisons, COs have unique perspectives on the success of gender-responsive strategies. Pendleton et al. (2020) assert that despite the COs’ responsibility of monitoring pregnant women in prison, as well as during labor and birth, their knowledge and perception of maternal and child health (MCH) policies and practices are largely unknown.
As such, in response to the lack of empirical research on prison COs’ knowledge on MCH programs, as well as the impact of such policies on COs’ primary job responsibility of maintaining safety and security, Pendleton et al. (2020) conducted a mixed-methods study “to understand COs’ knowledge and perceptions of programs and policies that support pregnant women in prison, with a specific emphasis on understanding COs’ perceptions of the [Minnesota Prison Doula Program (MnPDP)], a unique MCH program at the prison in which the research was conducted” (Pendleton et al., 2020, 3). Doulas are trained “companions” who support incarcerated pregnant women. While a handful of states employ doula programs, Pendleton et al. (2020) examined the MnPDP, which provides weekly parenting classes and one-on-one doula support to incarcerated women. Many prison systems, including Minnesota, do not allow family members or friends to attend the birth of an incarcerated women’s child; as such, Pendleton et al. (2020) argue that doulas are individuals who are “trained and experienced in childbirth who [provide] continuous physical, emotional, and informational support to the mother before, during and just after the birth,” doulas provide in-person support that pregnant women in prison cannot receive from family members or friends during labor and delivery” (Pendleton et al., 2020, 2).
The Pendleton et al. (2020) study was conducted with COs in the MnPDP through an online survey and in-person interviews to gain comprehensive qualitative and quantitative data. COs reviewed their knowledge and perspectives on policies available to pregnant women at the prison and whether policies had changed over time. The study’s findings add to the growing body of evidence that implementation of doula programs in carceral facilities have “CO support and may reduce job demands and stress for COs” (Pendleton et al., 2020, 9). Ultimately, the findings from this study suggest that MCH policies and programs for pregnant women also benefit COs by “reducing role conflict [which] may lead to higher CO approval and willingness to implement” (Pendleton et al., 2020, 9). For instance, 84% of COs agreed that the prison “provides the same standard of care or better care for pregnant offenders as the care non-incarcerated women would receive” (Pendleton et al., 2020, 4). Further, 34% of COs disagreed that “pregnant women should not be treated any differently than other women in prison,” and 76% disagreed that pregnant women should be restrained during labor and delivery (Pendleton et al., 2020, 4).
From the in-person interviews, the following five themes were derived from the comments made by COs:
“1) COs recognized that pregnancy poses a unique challenge to maintaining professional boundaries in prison; 2) COs perceived the prison doula program as benefitting pregnant women, infants, and their own work as COs; 3) Lack of training about the prison doula program made COs’ jobs more difficult; 4) COs had positive perceptions of the policy prohibiting the use of restraints on pregnant women in addition to concerns about policy implementation; 5) COs’ expressed varied perceptions of health services available to pregnant women” (Pendleton et al., 2020, 5).
COs also recognized that pregnancy poses a unique challenge to maintaining professional boundaries, as isolation from social support, as well as the lack of physical comforts, and separation from their infants can result in difficult conditions for women. The disconnect between empathy and professionalism was expressed by one officer, who noted that “there’s a natural barrier for me, where I can’t empathize with the offenders past a certain point, past a point that for me feels like a breach of professionalism” (Pendleton et al., 2020, 6). Similarly, another CO stated, “Anybody with any compassion wants to do something for her ‘Can I get you anything? Can I do anything?’, but in our job capacity we, I, shouldn’t be doing anything” (Pendleton et al., 2020, 6). Ultimately, the challenge to COs to remain professional is mitigated by MCH programs that include doulas. Doulas provided support to pregnant women outside of the COs’ job responsibilities, which dually allowed inmates to be supported while the COs maintained public safety.
Despite the aforementioned benefits of MCH programs and policies, there are noted limitations. For instance, many COs have argued that the lack of training on prison doula programs has created unnecessary difficulties in performing their job responsibilities. There is a significant lack of formal training: “COs stated that they had no knowledge of, or input into, the prison doula program when it began at the prison in 2010. Most COs expressed surprise or confusion regarding their first interactions with doulas” (Pendleton et al., 2020, 7). Ultimately, the lack of training added “awkwardness, uncertainty, and stress at the hospital” (Pendleton et al., 2020, 7) Additionally, there is a lack of formal systems in place for COs to identify pregnant women, which creates an issue when adhering to policies regarding pregnant inmates, especially those in early stages of pregnancy where it is harder to identify their condition. Regarding the restraint of pregnant inmates, the COs expressed that policies that prohibited the use of restraints “met women’s unique physical needs and did not interfere with COs’ role in maintaining security” (Pendleton et al., 2020, 8). As such, a beneficial future avenue for policy considerations would be to account for more comprehensive and informed training protocols for COs regarding MCH programs.
The study also noted that COs with a longer tenure recalled that prior to the implementation of MCH programs, many women lacked the emotional and physical support during labor and delivery that the prison doula system offers. The COs asserted that the doulas provided the “physical, emotional, and psychological support that women in labor needed while allowing COs to remain focused on their primary job responsibility of maintaining security, which reduced role conflict” (Pendleton et al., 2020, 9).
Ultimately, while the MCH programs offer gender-responsive programming for women inmates, they also raised ethical considerations. For instance, Pendleton et al. (2020) argue that some research has illustrated that prisons employing “enhanced MCH policies and programs may have a protective effect on certain clinical pregnancy outcomes, such as infant birth weight,” with COs arguing that the care available is of “higher quality compared to the availability of services in the community” (Pendleton et al., 2020, 10). Pendleton et al. (2020) argue that focusing solely on protective factors with prison MCH programs fails to address the broader social and structural health implications affecting the marginalized communities: “The reality is that many prisons in America have become de facto social service providers due to inadequate mental health, substance use, and social services available to marginalized pregnant women in the community” (Pendleton et al., 2020, 10). As such, viewing prisons as “protective” subsequently disregards the history of reproductive control and coercion experienced by racial and ethnic minority women.
Therefore, Pendleton et al.’s (2020) research asserts that COs’ perspectives should be incorporated into the creation and evaluation of MCH programming. As such, MCH programs have shown to improve conditions for both COs and incarcerated women. The study calls for future research to carefully study incarcerated pregnant women’s perspectives of the services they need, as well as community-based alternatives to incarceration. Pendleton et al. (2020) argue that to reduce the challenges that COs experience, implementing future MCH programs and policies with “robust training and opportunities for CO input will help ensure that programming optimally supports all key stakeholders” (Pendleton et al. 2020, 11). Finally, community-based programs that enter carceral spaces to “deliver MCH programming, such as prison doula programs or parenting support groups, may consider having a CO ‘champion’ within the facility to provide CO perspective and have a point person to help lead trainings” (Pendleton et al., 2020, 11). Ultimately, integrating COs’ views into the development and implementation of MCH programs and policies in prisons may improve facility safety and promote better maternal and child health.
References:
Daniel, R. (2019). [Picture of Statistics on Women in Prisons and Jails in 2017] [Digital Image]. Prison Policy Initiative. https://www.prisonpolicy.org/blog/2019/12/05/pregnancy/
Equal Justice Initiative. (2020, December 02). Shackling of pregnant women in jails and PRISONS continues in the United States. Retrieved April 24, 2021, from https://eji.org/news/shackling-of-pregnant-women-in-jails-and-prisons-continues/
Kupers, T. A. (1999). Chapter 1: The Mentally Ill Behind Bars. In Prison Madness The Mental Health Crisis Behind Bars and What We Must Do About It (pp. 9-38). San Francisco, CA: Jossey-Bass.
Pendleton, V., Saunders, J. B., & Shlafer, R. (2020). Corrections officers’ knowledge and perspectives of maternal and child health policies and programs for pregnant women in prison. Health & Justice, 8(1), 1-12. Retrieved April 24, 2021, from https://link.springer.com/article/10.1186/s40352-019-0102-0
Rousseau, D. (2021, April 06). Module 4 Study Guide. Blackboard. [Lecture notes].
Shine, N. (2016). [Picture of shackled pregnant inmate] [Photograph]. People Demanding for Action. https://www.peopledemandingaction.org/benefits-kitchen/item/491-new-jersey-lacks-law-addressing-shackling-of-pregnant-inmates-because-gov-christie-wouldn-t-sign-it
Sufrin, C. (2019). [Picture of Statistics on Pregnant Women in U.S. Prisons] [Digital Image]. John Hopkins Medicine. https://www.hopkinsmedicine.org/news/newsroom/news-releases/first-of-its-kind-statistics-on-pregnant-women-in-us-prisons