Zambia
Differentiated Service Delivery (DSD) was introduced to Zambia in 2013 in the form of standalone models and pilot projects offered by implementing partners. Since then, DSD has become a fundamental service delivery mechanism for the national ART program. To meet the needs of the healthcare system, Zambia identifies the nationwide availability of DSD services as a priority objective. The national program seeks to expand access to DSD models for stable clients as well as to prioritize models for adolescents.
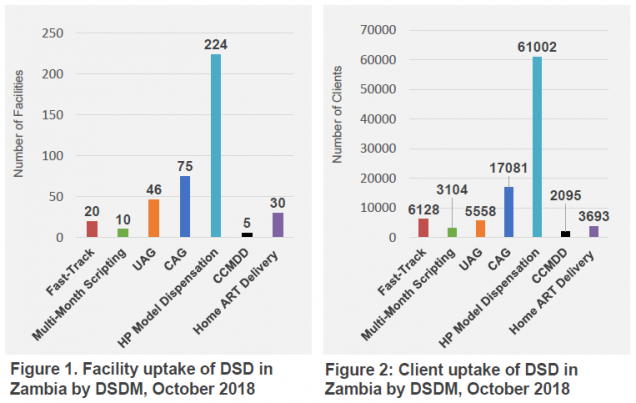
Currently nine DSD models for providing ART to the general adult patient are utilized in Zambia. These include:
- Three facility based models – Fast-Track, Multi-Month Scripting, and Urban/Rural Adherence Groups (UAG)
- Four community based models – Community Adherence Groups/Clubs (CAG), Chronic Centralized Medicines Dispensing & Distribution (CCMDD), Community Pharmacy Model, and Heath Post (HP) Model Dispensation
- Two outreach models – the Mobile ART Distribution Model and Home ART Delivery.
In addition to these, Zambia implements a model for adolescents and young adults, known as the Scholars (Adolescent) Model.
AMBIT in Zambia
We are now exploring the current extent of DSD implementation in Zambia, what is known about the scale of implementation, and the existing criteria for scale-up. For this purpose, we are identifying relevant data sources (publications, project databases, national EMR, etc.). Our next step will be to use available data on patient numbers and characteristics, facility locations, facility capacity, costs, and other variables to make recommendations about the most efficient combinations(s) of models of care to be implemented in each district.
Content adapted from: Lumano-Mulenga et al., Taking Differentiated Service Delivery to Scale in Zambia: A Coordinated Strategy to Increase Coverage. November, 2018